Plan C = Plan B: Revisiting the Labour Market's Role in Recovery
I have been revisiting old memories more frequently. Not stuck in the past per se, just simply finding ways to make sense of my present. One of the ways I like to do this, is read through old assignments and writings I had done years earlier. This one I am sharing with you, titled, Plan B: Contingencies for Canada’s Opioid Crisis I wrote for SPPH 550 – Public Health Approaches to Substance Use and Addictions during my time at the University of British Columbia in 2019. Our professor - Dr. Eugenia Oviedo-Joekes, Tier 1 Canada Research Chair In Person Centred Innovation In Addictions and Public Health - challenged students to choose a contemporary issue, critically evaluate the evidence, take a clear position, and propose a practical policy or implementation argument. After reading a book, Precarity: Uncertain, Insecure and Unequal Lives in Aotearoa New Zealand (gifted to me by Māori researchers that founded the He Pikinga Waiora Implementation Framework), I chose to question: could Canada's labour market play a larger role in substance use recovery? Seven years later, I'm revisiting that commentary, not to grade my younger self, but to ask what my life experience has taught me since.
Plan B: Contingencies for Canada’s Opioid Crisis
Canada’s opioid epidemic is felt deeply in our health systems, our economy, and in our hearts. In 2016, apparent opioid-related deaths in Canada reached 3,005, greater than the number of deaths due to the HIV epidemic in 1995 (“Opioid crisis having ‘significant’ impact on Canada’s health care system | CIHI,” 2018). More than 5,000 have died since, disproportionately killing our brothers, fathers, cousins, and uncles by accidental overdose (total of 9,000 by June 2018) (Canada, 2017). These stark numbers are a result of opioid availability in medical systems and potent synthetics infecting the street supply (e.g. fentanyl). Of deaths related to overdose, the percent of accidental overdose between January and September 2018 was 73%, steadily increasing from 54% in 2016 and 71% in 2017. As health systems, public health agencies, non-profits, and peers pool their reserves in an all hands on deck approach to save lives, research has failed to help one key player fully recognize their remedial role in substance use recovery: Canada’s labour market.
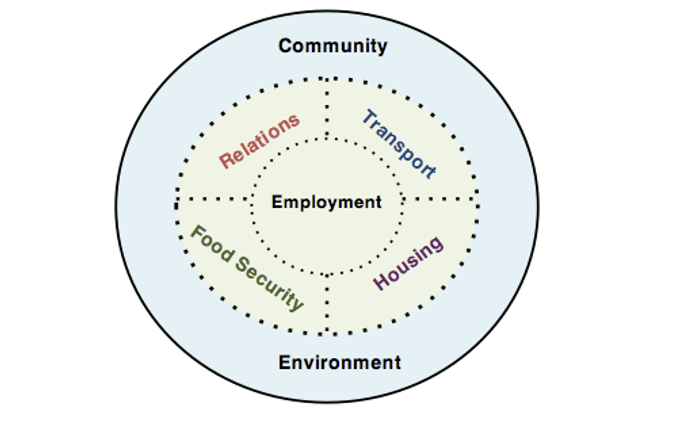
Figure 1. Employment as a core social determinant of health.
Employment is a social determinant of health at the core of housing affordability, building relationships, food security, and social inclusion (Figure 1) (Benach, Muntaner, & Santana, 2007; National Collaborating Centre for Aboriginal Health, 2017). Secure, long-term, and well-paid employment, in a workplace free of discrimination, improves health and reduces risk of substance use. Yet, access to the standard employment relations, trending post-WWII and the oil shocks of the 1970’s, has never been universal, remaining a gendered and racialized phenomena in Canada (Benach et al., 2014).
Current labour market trendsshow a tendency toward increasing employment precarity(Vosko, 2006). Precarity indicators routinely measured by Statistics Canada (defined by wage, full time status, access to extended health coverage) do not currently capture the array of workplace conditions that we know influence health. While employment may be packaged as “flexible”, the non-standard and temporary arrangements are more likely to offer fewer protections, lower wages and/or minimal extended benefits. Job quality in Canada was assessed using a more multidimensional approach in December 2018, with results supporting perceived precarity affiliated with the increase in non-standard employment, including seasonal, fixed-term, and casual workers. These contracts are associated with lower pay, low job security, and other characteristics that disadvantage workers health (Chen, Mehdi, Statistics Canada, & Analytical Studies Branch, 2018). Groups at risk of non-standard work (voluntarily or involuntarily) were also identified (women, youth, less-educated). Finally, trends toward a lack of enforcement of the Employment Standards Actas temporary work increases is cited as a major threat to workplace safety and employee working conditions (Longhurst & Canadian Centre for Policy Alternatives, 2014).
First Nations in Canada were the hardest hit during the Great Recession, and have seen their largest growth in employment in non-standard categories (National Collaborating Centre for Aboriginal Health, 2017). Rates of self-employment, especially for on-reserve First Nations, have steadily increased. While on-reserve work can contribute to a known protective factor (e.g. retaining connection to land, culture, & traditional healing) by allowing individuals or families to remain in their traditional territory, nearly half of status First Nations live off-reserve today. Labour market experiences of off-reserve status First Nations also highlights the challenges of finding work due to shortage of jobs or lack of work experience required by many employers in both rural and urban regions (Government of Canada, 2018). In the workplace, First Nations workers still face higher rates of racism and discrimination, known risk factors a myriad of poor health outcomes including substance use. Despite strong associations between employment and health, research has historically failed to link causes of premature mortality in First Nations to labour force status (National Collaborating Centre for Aboriginal Health, 2017).
The legacy of colonization has contributed to the current opioid crisis and its disproportionate effect on First Nations (First Nations Health Authority, n.d.). In British Columbia, preliminary findings during the opioid crisis found First Nations were five times more likely than non-First Nations to experience an opioid overdose event and three times more likely to die due to overdose (First Nations Health Authority, n.d.). Amidst our health services sector, they are twice as likely to be dispensed an opioid, but report struggling with access to a safe supply longer-term from trusted medical professionals. While communities and health professionals advocate for safe supply and financial supports in a reactionary approach, the Union of BC Indian Chiefs still seeks justice for the healing and recovery of First Nations and their communities from the harms imposed by medical and pharmaceutical industry (March 11, 2019, n.d.). How will the levels of government be proactive to ensure First Nations are not disproportionately affected by crises, from recession to tainted drug supply, in the future?
Current research into workplace policy and assessing how employers in Canada actually support individuals with substance use is in its infancy. The Canadian Centre on Substance Use & Addiction (CCSA) released the first study of its kind to explore the state of Canadian substance use policies in the workplace in spring of 2018, to be followed by a report focused on substance use-related costs borne by employers (Meister, 2018). The targeted organizations in the study (N=35) were believed to have comprehensive substance use policies (comprehensive = at least 6 of 8 identified themes). However, it was found mostly safety-sensitive employers had comprehensive policy, although most measures were in place for termination and few focused on supportive elements (i.e. employer referring employee to assistance program). While the Joint Statement of Action to Address the Opioid Crisis: A Collective Response from Health Canada and the CCSA indicates support to enhance collaboration across sectors that influence the social determinants of health, they do not explicitly state partnerships with the labour market (Health Canada & Canadian Centre on Substance Use and Addiction, 2016). And while the federations of labour have cited impactsof the opioid epidemic on economic outputs and safety, there has been no statement of the labour markets role in contributing to a solution. We know the importance of employment as a key social determinant of health but fail to mobilize this knowledge to action.
Research highlights the need to assess job growth while considering job quality, necessary for decision-makers to understand the full extent to which the labour market further disadvantages at-risk populations like First Nations, and the impacts on the development of a robust and inclusive economy. Assessing job growth will be a timely undertaking. In crisis, we must ask critical questions and look to research and policy to take reasonable action that is truly multidisciplinary. For example, we can ask: how can employment support recovery for unemployed, opioid-dependent populations during the opioid epidemic?
Therapeutic Workplace (TW) researchers evaluate training and employment interventions for chronically unemployed, opiate-dependent populations. TW incorporates contingency management (CM), a well-cited behavioural therapy that uses reinforcers (e.g. money/vouchers) to strengthen behavioural change. It’s the furthest look into long-term abstinence maintenance that combines vocational training, employment, and CM. Adults who participated in job skills training and employment, rewarded on attendance and productivity, were more likely to abstain from opiate use, continue methadone treatment, and find employment (Aklin et al., 2014; Subramaniam et al., 2018). However, once the intervention was discontinued, many effects were not sustained. Community Reinforcement Approaches (CRA) focus on providing positive reinforcements for people who use substances in their environments that are incompatible with drug use (e.g. improving family relations). Evidence across multiple randomized controlled trials indicates that CRA + incentives is more effective for cocaine and opiate abstinence than usual care or CRA alone (Roozen et al., 2004). There is strong evidence for CM for opiate and cocaine use recovery, with promise of success in clinics or community-based settings (CRA or TW) (Roll, Madden, Rawson, & Petry, 2009). CM in our labour market could complement the suite of effective treatment options offered by clinics. So, why is it rarely implemented?
Reinforcers requiring drug testing pose an ethical barrier. For example, the Human Rights Commission suggests urine sampling be reserved for safety-sensitive workplaces (Els, Jackson, Milen, Kunyk, & Straube, 2018). Arguably, there are ethical concerns around having a highly effective treatment for a population that fails to materialize. Could there be a clause related to CM in the workplace to prevent deaths by accidental overdose? Practical application is also complex. We need willing employers with supports for training and reporting for accountability. And reinforcers must be salient, timely applied, and of low-cost.
A comprehensive review of the literature can inform implementation of evidence-based reinforcers. But what effectiveness research lacks can also be captured through rigorous evaluation or implementation. Implementation research that engages people who use substances alongside key implementers informs timely modifications (Bernet, Willens, & Bauer, 2013). Systematically evaluating the implementation, alongside effectiveness research or on its own, using pragmatic methods can provide understandings that decades of research in this field have only partially achieved.
To fully realize the therapeutic role of the labour market during crisis, researchers can begin by:
1.) Defining and advocating for measures of precarity that best inform health research of vulnerable populations.
2.) Defining and advocating for outcome measures meaningful for Canadian employees and communities (e.g. supportive workplace policy and level of enforcement) to be captured and translated beyond just indicators of productivity or disability.
3.) Developing targeted, evidence-based CM implementation strategies that promote re-integration of people who use opiates in the labour market.
Increasing employment rates when we cannot define precarity or fail to recognize employment as a key determinant of health for our citizens does little for the most vulnerable. When drug supplies are tainted, maintaining long-term abstinence in recovery can save lives. If this is our primary goal during an epidemic, it’s worth learning if mobilizing CM in our communities is a viable Plan B.
What seven years has taught me about work and recovery.
In 2019, I had argued that Canada had overlooked one of the most powerful social determinants of health in responding to the opioid crisis: employment. I went over my 10 minute allocation for my presentation. We were all nervous during her question period - she knew how to ask the tough ones.
Dr. Oviedo-Joekes stumped me with a question I will never forget: How would you explain everything you just said to us, to a room with Conservatives? She then explained to us all the challenges she and her research team face in operationalizing support for people facing addiction and substance use struggles, with papers denied often by renowned peer-reviewed journals. She said, “If your thinking is before its time it is often harder to operationalize.”
At 26, it was the most important lesson. It was also a time where I watched a family member relapse into a system where addiction and substance use support was dismal. I was attending classes and visiting a family member in recovery homes in Surrey, where the success rates of recovery were as low as 4%. In a world where we’ve suggested everything we can, from harm reduction and safe supply to housing and treatment facilities - what else can we do?
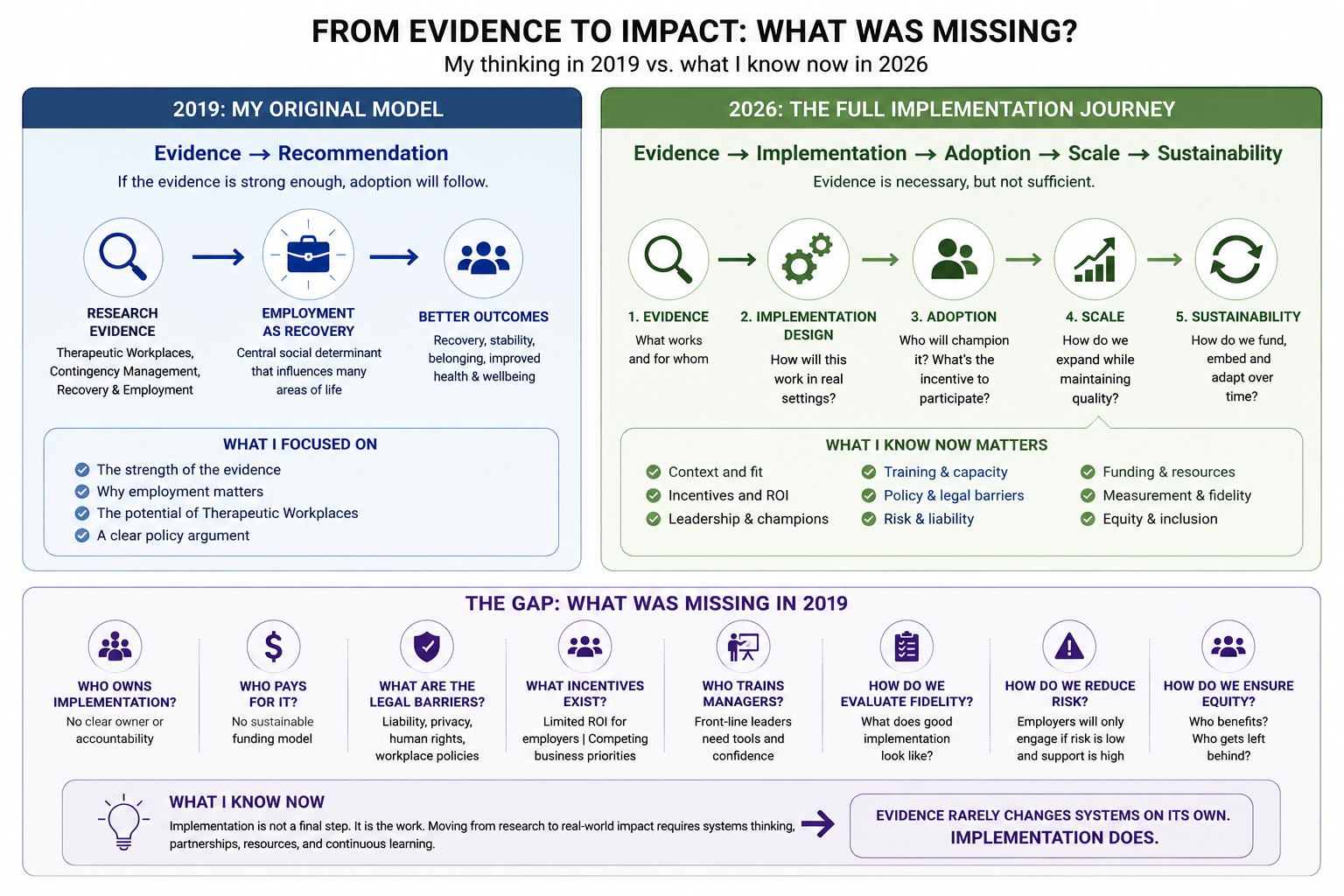
Coming from a place of helplessness likely fueled how deeply I immersed myself in this coursework. I believed that if the evidence was strong enough, implementation would naturally follow along with my recommendations listed. I was only beginning to understand theories of change, implementation science, and organizational behaviour. I hadn't yet spent years managing budgets, hiring staff, writing grants, navigating policy, or balancing competing priorities in a resource-constrained organization. Today, I see why asking employers to adopt contingency management isn't simply a question of evidence and metrics. It's a question of incentives, capacity, liability, culture, leadership, and risk. The implementation challenge was always much bigger than I appreciated.
Proving an idea to engineering its adoption
I left graduate school believing policy was primarily about identifying the right intervention. The years that followed taught me something different. Working in local government, I discovered that organizations rarely ask, "Does the evidence support this?" More often, they ask, "Can we realistically deliver it?"
Every new program competes with limited staff time, finite budgets, organizational risk, reporting requirements, competing priorities, and community expectations. Even when the evidence is compelling, the easiest thing to implement is often what already exists. Innovation takes time, leadership, funding, and people willing to champion an idea long after the research has been published.
As Recreation Coordinator for Haida Gwaii Recreation, I have found myself on both sides of that equation. I've advocated for evidence-informed programs while simultaneously wrestling with staffing shortages, grant deadlines, operational budgets, and the reality that every new initiative carries opportunity costs. The question is no longer simply, "Does this work?" It's "How do we make it work within the system we actually have?"
Looking back, I realize my 26-year-old self focused almost entirely on the intervention. Today, I spend just as much time thinking about implementation. The intervention may be evidence-based, but adoption depends on incentives, organizational capacity, partnerships, leadership, and trust. In many ways, implementation has become the intervention.
Made with support by ChatGPT.
When I attempted to publish the commentary, the feedback was constructive but clear. The argument needed to engage more deeply with implementation, particularly the unique impacts of substance use, employment, and colonialism on First Nations communities. Before I had the opportunity to revise and resubmit, life took a different direction.
In 2018, I met my partner, moved back to Haida Gwaii, and began my career in recreation. Academic publishing quietly moved to the background as I focused on building a life and a career. Instead, I found another outlet for my ideas through a blog under my business name, Pacific Chiton Consulting, where I continued writing about public policy, public health, and community development.
Looking back, I am grateful the paper was never published in its original form. The central idea that employment plays a critical role in recovery has become increasingly recognized. By 2026, contingency management had moved from the margins toward mainstream addiction policy, supported by a growing body of evidence and broader implementation efforts, including works led by Dr. Eugenia Oviedo-Joekes. Fascinating to her outcomes in this research? Being at work was therapeutic.
I had focused on proving that an intervention worked. I had given far less attention to the organizational, political, and economic conditions required for it to be adopted. I underestimated the implementation burden. Evidence alone does not change systems. Organizations need capacity, incentives, leadership, funding, partnerships, and time before evidence becomes practice.
In many ways, this assignment shaped the next chapter of my career. It sparked an enduring interest not only in what works, but in how ideas move from research into organizations and communities. Looking back, I can trace a direct line from this paper to my work in recreation, my growing interest in implementation science and systems change, and eventually to pursuing an MBA.
My questions did not move away from research. They evolved from asking, “What works?” to asking, “How do we make what works possible?”
Employment remained central to that evolution. It is one of the most powerful social determinants of health, shaping income, identity, purpose, belonging, stability, and access to opportunity. As I moved into management, I began asking a related question from the other side: what does healthy employment look like?
What kinds of workplaces help people recover, grow, contribute, and remain well? How do we support staff before they reach a crisis? How do we create organizations that recognize the realities of addiction, disability, caregiving, trauma, and difference without lowering expectations or abandoning accountability? Those questions became increasingly important in my own work. I was no longer only interested in whether employment could support health. I want to understand how workplaces themselves could become healthier, more responsive, and more capable of helping people succeed.
Plan B = Plan C
So where are we now? Contingency management is no longer a fringe idea. Decades of research have demonstrated that it works, and in Canada, the Canadian Research Initiative in Substance Misuse (CRISM) has developed practical guidance for implementing contingency management within healthcare settings. The conversation has shifted from asking whether contingency management works to asking how healthcare organizations can successfully adopt it.
Yet one important question remains largely unanswered. How do we move beyond healthcare?
My original paper argued that employment itself could be a powerful component of recovery. Today, I would ask a different question: how do we create labour markets and workplaces that actively support recovery rather than simply accommodate it?
The therapeutic workplace remains an intriguing but underdeveloped concept in Canada. The challenge is no longer behavioural science. It is organizational behaviour. Why would an employer choose to invest in becoming a recovery-supportive workplace? What incentives exist? How do we reduce perceived risks while increasing the value for businesses, employees, and society? The solution never really changed. Plan C became finding a way to make Plan B possible.
What has evolved since 2018 is my understanding of implementation. The next frontier is not proving that contingency management works. It is engineering the conditions that allow it to succeed outside research studies and healthcare settings. That means asking how governments, insurers, employers, and communities can align incentives to support recovery through meaningful employment.
Perhaps that means tax incentives for employers who invest in recovery-supportive practices. Perhaps it means wage subsidies, insurance premium reductions, procurement incentives, or recognition programs for organizations that demonstrate leadership in workplace recovery. Whatever the mechanism, the question is no longer simply how to change individual behaviour. It is how to design systems that make the desired behaviour easier, more attractive, and ultimately sustainable.
The opioid crisis has only intensified since I wrote that paper. Debates over safe supply, decriminalization, and treatment continue to dominate public discourse. Yet we spend far less time asking how the places where Canadians spend much of their lives—their workplaces—might become part of the solution. If employment is one of the most powerful social determinants of health, then healthy workplaces should be considered an essential part of our public health infrastructure.
If I were to present this work to Dr. Oviedo-Joekes today, I think my answer to her question would be different. In 2018, she challenged me to explain my ideas to "a room full of Conservatives." Today, I would answer that productivity may be one of the few truly non-partisan policy languages available to us.
Framing recovery-supportive workplaces that incorporate evidence-based practices such as contingency management as investments in productivity, employee retention, workforce resilience, and long-term organizational performance may help bridge ideological divides in ways that public health arguments alone sometimes cannot. The question is no longer simply whether supporting recovery is the right thing to do. It is whether we can demonstrate that healthier workplaces are also more productive, more resilient, and ultimately better for employees, employers, and society alike.
Perhaps that is how I would answer Dr. Oviedo-Joekes today. Not by changing the evidence, but by changing the language through which we communicate it. Sometimes the most effective way to advance a public health idea is to show that it is also sound economic policy.
With Thanks
This paper began as a graduate school assignment. I never imagined it would become something I would revisit nearly a decade later. Thank you to Dr. Eugenia Oviedo-Joekes for creating a classroom where difficult questions were welcomed, unconventional ideas were challenged, and students were encouraged to think beyond the evidence and into the realities of implementation. Your mentorship shaped not only how I approached research, but how I now approach leadership, organizations, and systems change.
Thank you for supporting my journey from public health to business administration. Looking back, I realize I never really left public health behind. I simply found another language through which to pursue it.
Finally, thank you to the family member whose recovery inspired this work in the first place. Your resilience taught me more about hope than any textbook ever could.
This paper was never published, but it changed the questions I spent the next decade trying to answer.
References (Plan B Commentary):
Aklin, W. M., Wong, C. J., Hampton, J., Svikis, D. S., Stitzer, M. L., Bigelow, G. E., & Silverman, K. (2014). A Therapeutic Workplace for the Long-Term Treatment of Drug Addiction and Unemployment: Eight-Year Outcomes of a Social Business Intervention. Journal of Substance Abuse Treatment, 47(5), 329–338. https://doi.org/10.1016/j.jsat.2014.06.013
Benach, J., Muntaner, C., & Santana, V. (2007). Employment Conditions and Health Inequalities. Final Report to the WHO. (pp. 1–172). Retrieved from Employment Conditions Knowledge Network (EMCONET) website: https://www.who.int/social_determinants/resources/articles/emconet_who_report.pdf?ua=1
Benach, J., Vives, A., Amable, M., Vanroelen, C., Tarafa, G., & Muntaner, C. (2014). Precarious Employment: Understanding an Emerging Social Determinant of Health. Annual Review of Public Health, 35(1), 229–253. https://doi.org/10.1146/annurev-publhealth-032013-182500
Bernet, A. C., Willens, D. E., & Bauer, M. S. (2013). Effectiveness-implementation hybrid designs: implications for quality improvement science. Implementation Science, 8(1), S2. https://doi.org/10.1186/1748-5908-8-S1-S2
Canada, H. (2017, September 14). Opioid-related harms and deaths in Canada [Datasets]. Retrieved April 11, 2019, from aem website: https://www.canada.ca/en/health-canada/services/substance-use/problematic-prescription-drug-use/opioids/data-surveillance-research/harms-deaths.html
Chen, W.-H., Mehdi, T., Statistics Canada, & Analytical Studies Branch. (2018). Assessing job quality in Canada: a multidimensional approach. Retrieved from http://epe.lac-bac.gc.ca/100/201/301/weekly_acquisitions_list-ef/2018/18-50/publications.gc.ca/collections/collection_2018/statcan/11f0019m/11f0019m2018412-eng.pdf
Els, C., Jackson, T. D., Milen, M. T., Kunyk, D., & Straube, S. (2018). Random drug and alcohol testing for preventing injury in workers [Protocol]. Cochrane Database of Systematic Reviews 2018.
First Nations Health Authority. (n.d.). Overdose Data and First Nations in BC: Preliminary Findings (pp. 1–16). Retrieved from http://www.fnha.ca/newsContent/Documents/FNHA_OverdoseDataAndFirstNationsInBC_PreliminaryFindings_FinalWeb.pdf
Government of Canada, S. C. (2018, November 26). Labour market experiences of First Nations people living off reserve: Key findings from the 2017 Aboriginal Peoples Survey. Retrieved April 10, 2019, from https://www150.statcan.gc.ca/n1/pub/89-653-x/89-653-x2018003-eng.htm
Health Canada, & Canadian Centre on Substance Use and Addiction. (2016). Joint Statement of Action to Address the Opioid Crisis: A Collective Response (pp. 1–24). Retrieved from http://www.ccsa.ca/Resource%20Library/CCSA-Joint-Statement-of-Action-Opioid-Crisis-Annual-Report-2017-en.pdf
Longhurst, A., & Canadian Centre for Policy Alternatives. (2014). Precarious temporary agency work in British Columbia. Retrieved from http://www.deslibris.ca/ID/243464
March 11, E. N. 69sc on, & 2019. (n.d.). UBCIC Recognizes Opioid Crisis as “A State of Emergency.” Retrieved April 11, 2019, from UBCIC website: https://www.ubcic.bc.ca/ubcic_recognizes_opioid_crisis_as_a_state_of_emergency
Meister, S. R. (2018). A Review of Workplace Substance Use Policies in Canada: Strengths, Gaps and Key Considerations (pp. 1–90). Retrieved from Canadian Centre on Substance Use and Addiction20180104 website: http://www.ccsa.ca/Resource%20Library/CCSA-Workplace-Substance-Use-Policies-Canada-Report-2018-en.pdf
National Collaborating Centre for Aboriginal Health. (2017). Employment as a Social Determinant of First Nations, Inuit and Métis Health (pp. 1–20). Retrieved from https://www.nccah-ccnsa.ca/495/Employment_as_a_social_determinant_of_First_Nations,_Inuit_and_M%C3%A9tis_health.nccah?id=228
Opioid crisis having “significant” impact on Canada’s health care system | CIHI. (2018, July 4). Retrieved December 3, 2018, from https://www.cihi.ca/en/opioid-crisis-having-significant-impact-on-canadas-health-care-system
Roll, J. M., Madden, G. J., Rawson, R., & Petry, N. M. (2009). Facilitating the Adoption of Contingency Management for the Treatment of Substance Use Disorders. Behavior Analysis in Practice, 2(1), 4–13. https://doi.org/10.1007/BF03391732
Roozen, H. G., Boulogne, J. J., Tulder, M. W. van, Brink, W. van den, Jong, C. A. J. D., & Kerkhof, A. J. F. M. (2004). A systematic review of the effectiveness of the community reinforcement approach in alcohol, cocaine and opioid addiction. Drug & Alcohol Dependence, 74(1), 1–13. https://doi.org/10.1016/j.drugalcdep.2003.12.006
Subramaniam, S., Holtyn, A. F., Jarvis, B. P., Koffarnus, M. N., Leoutsakos, J. S., & Silverman, K. (2018). Illicit drug use and work in a model therapeutic workplace. Drug and Alcohol Dependence, 191, 110–116. https://doi.org/10.1016/j.drugalcdep.2018.06.019
Vosko. (2006). Precarious Employment: Understanding Labour Market Insecurity in Canada. McGill-Queen’s Press - MQUP.